The Behavioral Health Landscape in Michigan
Michigan is facing a severe access crisis for mental health and substance use disorder (SUD) services, a situation worsened by the COVID-19 pandemic. 2019 data indicates that nearly half of Michigan adults with mental illness and 73% of those with SUD do not receive treatment. A critical takeaway from the brief is that insurance coverage does not guarantee access to care.
Systemic Challenges
- Workforce Shortages: Approximately 6 million residents live in Mental Health Professional Shortage Areas. The state needs at least 249 more psychiatrists to alleviate these gaps.
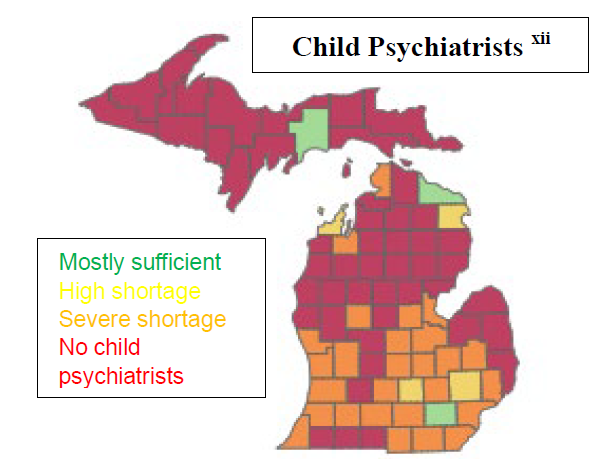
- Pediatric Crisis: Michigan has only 11 child psychiatrists per 100,000 people, significantly below the recommended ratio of 47.
- Wait times and “ED Boarding”: Insufficient outpatient providers and inpatient beds lead to long waitlists and “ED boarding,” where patients wait days in emergency departments for psychiatric care.
- Payment Barriers: Many outpatient providers do not accept insurance, forcing patients to pay out-of-pocket even when covered.
Current Coverage Structure
The system is divided by the severity of the patient’s needs:
- Mild-to-Moderate: Covered by private insurance, Medicare Part B, or Medicaid health plans.
- Moderate-to-Serious: Managed through a Medicaid “carve out” via Prepaid Inpatient Health Plans (PIHPs) and Community Mental Health (CMH) programs.
Desired Outcomes and Strategic Solutions
To bridge these gaps, the brief proposes several strategic interventions:
- Funding loan repayment programs and scholarships for behavioral health education and training.
- Increasing residency slots for psychiatrists and utilizing visa waiver programs (Conrad30) for foreign medical graduates.
- Expanding the “scope of practice” to allow nurse practitioners and physician assistants to perform evaluations and treatments at the “top of their licenses”.
- Joining interstate licensing compacts to streamline the licensure process and reduce barriers to practice.
2. Integrated Care and Community Services
- Expanding Certified Community Behavioral Health Clinics (CCBHCs) and behavioral health homes to integrate physical and mental health care.
- Supporting collaborative care models like Michigan Child Collaborative Care (MC3), where specialists support primary care providers in delivering services.
- Continuing efforts to “carve back in” behavioral health services to Medicaid health plans to improve financial integration.
3. Policy and Reimbursement
- Parity Enforcement: Strictly enforcing federal laws requiring mental health coverage to be no more restrictive than physical health coverage.
- Telehealth Support: Ensuring permanent and adequate reimbursement for behavioral health telehealth services across all insurance types.
The ultimate goal is a coordinated, adequately staffed system that eliminates geographic and financial barriers to ensure timely care for all residents.