Advancing the Profession and Sustainability of Community Health Workers
 Community Health Workers (CHWs) strive to bridge gaps between traditional healthcare providers and the communities they serve, but the community health worker profession faces several challenges to realizing its full potential. In the fall of 2017, the Center for Healthcare Research and Transformation (CHRT) published an issue brief that focused on the ways State Innovation Model (SIM) grants have helped regions across the nation integrate community health workers into their healthcare systems. In this issue brief, CHRT enumerates the challenges states and health systems will need to overcome as they seek to develop a sustainable revenue stream for this work, to advance the community health worker profession, and to amplify the impact.(1)J. Lapedis, E. Kieffer, and M. Udow-Phillips, Revisioning the Care Delivery Team: The Role of CHWs within State Innovation Models (Ann Arbor, MI: Center for Healthcare Research & Transformation, Nov. 2017): Revisioning the Care Delivery Team: The Role of CHWs within State Innovation Models | Center for Health & Research Transformation (chrt.org)
Community Health Workers (CHWs) strive to bridge gaps between traditional healthcare providers and the communities they serve, but the community health worker profession faces several challenges to realizing its full potential. In the fall of 2017, the Center for Healthcare Research and Transformation (CHRT) published an issue brief that focused on the ways State Innovation Model (SIM) grants have helped regions across the nation integrate community health workers into their healthcare systems. In this issue brief, CHRT enumerates the challenges states and health systems will need to overcome as they seek to develop a sustainable revenue stream for this work, to advance the community health worker profession, and to amplify the impact.(1)J. Lapedis, E. Kieffer, and M. Udow-Phillips, Revisioning the Care Delivery Team: The Role of CHWs within State Innovation Models (Ann Arbor, MI: Center for Healthcare Research & Transformation, Nov. 2017): Revisioning the Care Delivery Team: The Role of CHWs within State Innovation Models | Center for Health & Research Transformation (chrt.org)
Key challenges
Numerous studies have demonstrated the significant value of community health workers,(2)L. M. Gottlieb et al., “Effects of Social Needs Screening and In-Person Service Navigation on Child Health: A Randomized Clinical Trial,” JAMA Pediatrics 170, no. 11 (Nov. 7, 2016): e162521, doi:10.1001/jamapediatrics.2016.2521 but several obstacles stand in the way of their widespread adoption and continued development. In this brief, we outline some of the most significant challenges and describe how leaders across the nation are working to overcome them:
- Scope. Many healthcare professionals are unfamiliar with the skills community health workers bring to health care teams. While most recognize their value as translators between health care professionals and the communities they serve, community health workers bring many other abilities. Promoting the diverse scope of skills community health workers can offer is essential to realizing their full potential.
- Training. Community health worker training and certification processes vary around the country. Formalizing this process would provide employers and payers with assurance that community health workers have achieved a standard set of core competencies related to their roles.
- Integration. Community health workers can play many different roles in health systems, which presents challenges for payers and employers who are working to integrate them into existing teams. While community health workers have proven particularly effective at working with narrowly defined populations or addressing specific programmatic goals, they should be given time to work in the community and to help their patients navigate a broader range of health and social concerns.
- Funding. The funding mechanisms most commonly used to support community health workers—largely grants from government and foundation sources that support short-term work with individual patients—provide unstable revenue streams that can disrupt demonstrated improvements in individual and community health outcomes, and community health worker careers. While some health systems and health plans have begun financing community health workers for short-term interventions with high-cost patients, sustainable financing is not yet available for CHW services where cost-savings take longer to achieve (health promotion, maternal and infant health, disease prevention, and self-management).
Methods
The authors conducted in-depth, qualitative interviews with key informants from 14 states. The 19 informants included state health department and Medicaid officials, leaders of state community health worker associations, leaders in health systems and other organizations employing community health workers, and community health workers themselves. The authors supplemented these interviews with a literature review including academic and non-academic publications, as well as a landscape analysis of state policies.
1. Defining community health worker roles
There is no singular definition of a community health worker (CHW).(3)To date, the most widely used definition is from the American Public Health Association: “A community health worker is a frontline public health worker who is a trusted member of and/or has an unusually close understanding of the community served. This trusting relationship enables the worker to serve as a liaison/link/intermediary between health/social services and the community to facilitate access to services and improve the quality and cultural competence of service delivery.” American Public Health Association, “Community Health Workers,” 2017, https://www.apha.org/apha-communities/member-sections/community-health-workers. CHWs are employed by a variety of organizations—large health plans, local health departments, federally qualified health centers, social service organizations, and more. Each organization specifies community health worker roles, and leverages their skills in different ways, but not all take advantage of the full scope of roles and skills that CHWs can offer.
The experts interviewed for this brief shared three common attributes of effective community health workers:
- The capacity to harness shared experiences to build trust
 with patients, to improve healthcare and human service systems navigation, and to anticipate potential barriers to addressing health and social needs.
with patients, to improve healthcare and human service systems navigation, and to anticipate potential barriers to addressing health and social needs. - The capacity to serve as a cultural bridge between patients and providers, so that providers are better able to understand patients’ health problems and adapt their services to better serve patients.
- The ability to advocate on behalf of patients, helping to change the systemic policies and practices that get in the way of improved health and access to care.
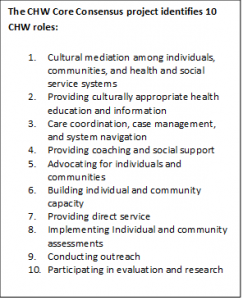
While these three qualities are key, community health workers can play many other important roles. The CHW Core Consensus (C3) project, a national effort to advance consensus on CHW scope of service and competencies, has enumerated 10 roles (above right).(4)E. Rosenthal, C. Rush, and C. Allen, Understanding Scope and Competencies: A Contemporary Look at the United States Community Health Worker Field (University of Texas-Houston School of Public Health, April 2016): http://www.healthreform.ct.gov/ohri/lib/ohri/work_groups/chw/chw_c3_report.pdf Some of these focus on individualized services that can be offered to patients, while others focus on community-level or systemic change efforts. By taking a broader view of the roles community health workers can fill, their host organizations can tap into their full potential.(5)A. Olaniran et al., “Who Is a Community Health Worker? A Systematic Review of Definitions,” Global Health Action 10, no. 1 (Jan. 2017): 1272223, https://doi.org/10.1080/16549716.2017.1272223.
2. Formalizing the community health worker profession
Despite a long history in other countries,(6)L. Pérez and J. Martinez, “Community Health Workers: Social Justice and Policy Advocates for Community Health and Well-Being,” American Journal of Public Health 98, no. 1 (Jan. 2008): 11–14: https://doi.org/10.2105/AJPH.2006.100842 and employment in the United States since the 1960s, the community health worker (CHW) profession is not yet formalized in this country. Unlike other healthcare professions, most CHW training is conducted by employers, health systems, or health plans, and does not lead to state-recognized certification. Formalizing the role of community health workers would help clinical providers understand how CHWs can complement their own strengths and fit into their practice workflows. Formalization also enables employers and payers to have more assurance that community health workers have achieved a standard set of core competencies related to their roles. Finally, more standardized training and certification processes may provide CHWs with greater employment opportunities due to the transferability of their basic skill set among settings.
Though no state has mandatory community health 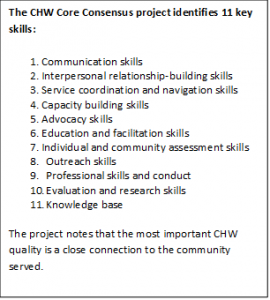 worker certification, 13 states have voluntary certification programs and 11 others are exploring the feasibility of statewide community health worker certification.(7)National Academy for State Health Policy, State Community Health Worker Models, National Academy for State Health Policy, Aug. 2017: http://nashp.org/state-community-health-worker-models/ Nine states have official training and certification programs, while several others have state statutes or advisory boards that establish training curricula.(8)National Academy for State Health Policy, State Community Health Worker Models, National Academy for State Health Policy, Aug. 2017: http://nashp.org/state-community-health-worker-models/ In Minnesota, for example, community health worker training programs are standardized across the state. In Oregon, Ohio, and Wisconsin, several training programs are recognized for certification. In other states, training programs are required to follow a set of core competencies—like those identified by the CHW Core Consensus project (above right).(9)Rosenthal, Rush, and Allen, “Understanding Scope and Competencies: A Contemporary Look at the United States Community Health Worker Field.” Altogether, 20 states have core competencies or state-endorsed training programs.(10)National Academy for State Health Policy, State Community Health Worker Models, National Academy for State Health Policy, Aug. 2017: http://nashp.org/state-community-health-worker-models/
worker certification, 13 states have voluntary certification programs and 11 others are exploring the feasibility of statewide community health worker certification.(7)National Academy for State Health Policy, State Community Health Worker Models, National Academy for State Health Policy, Aug. 2017: http://nashp.org/state-community-health-worker-models/ Nine states have official training and certification programs, while several others have state statutes or advisory boards that establish training curricula.(8)National Academy for State Health Policy, State Community Health Worker Models, National Academy for State Health Policy, Aug. 2017: http://nashp.org/state-community-health-worker-models/ In Minnesota, for example, community health worker training programs are standardized across the state. In Oregon, Ohio, and Wisconsin, several training programs are recognized for certification. In other states, training programs are required to follow a set of core competencies—like those identified by the CHW Core Consensus project (above right).(9)Rosenthal, Rush, and Allen, “Understanding Scope and Competencies: A Contemporary Look at the United States Community Health Worker Field.” Altogether, 20 states have core competencies or state-endorsed training programs.(10)National Academy for State Health Policy, State Community Health Worker Models, National Academy for State Health Policy, Aug. 2017: http://nashp.org/state-community-health-worker-models/
While interviewees supported formalizing the certification and training process for community health workers, it is important to note that they also cautioned against rigid requirements that act as barriers to community health workers in practice. Alternatives to state-regulated certification include community health worker registries, which may allow for more flexibility in the registration process. One notable example is the Michigan Community Health Worker Alliance registry, a statewide database of community health workers who have achieved core competencies through training or experience.
Ultimately, experts interviewed for this brief believed that effective training programs needed to balance two challenges. First, community health worker training programs need to be understood by those outside the profession. This ensures legitimacy and clarifies how community health workers fit into the context of larger health systems. Second, training programs must draw upon the real-world experiences of community health workers, who have learned which skills are core to successful practice.(11)N. Wiggins et al., “Preparing Community Health Workers for Their Role as Agents of Social Change: Experience of the Community Capacitation Center,” Journal of Community Practice 21, no. 3 (July 2013): 186–202 Placing more emphasis on a training program that is legitimate in the eyes of those outside the profession runs the risk of marginalizing the role of experienced community health workers and missing important lessons that only veteran CHWs can teach. These two requirements can be complementary in a carefully designed training program.
3. Integrating community health workers into health systems
Community health workers (CHWs) play many different roles across programs.(12)For a table outlining the different CHW roles in State Innovation Models across the United States, see our companion brief: J. Lapedis, E. Kieffer, and M. Udow-Phillips, Revisioning the Care Delivery Team: The Role of CHWs within State Innovation Models (Ann Arbor, MI: Center for Healthcare Research & Transformation, Nov. 2017): https://chrt.org/publication/revisioning-care-delivery-team-role-chws-within-state-innovation-models. This variation can pose challenges for integrating them into formal healthcare systems due, in part, to a general lack of knowledge about the skills community health workers possess,(13)M. Shah, M. Heisler, and M. Davis, “Community Health Workers and the Patient Protection and Affordable Care Act: An Opportunity for a Research, Advocacy, and Policy Agenda,” Journal of Health Care for the Poor and Underserved 25, no. 1 (2014): 17–24, https://doi.org/10.1353/hpu.2014.0019; J. Payne et al., “Integrating Community Health Workers (CHWs) into Health Care Organizations,” Journal of Community Health, April 8, 2017: https://doi.org/10.1007/s10900-017-0345-4. as well as concerns about standards of care.(14)A. Witmer et al., “Community Health Workers: Integral Members of the Health Care Work Force.,” American Journal of Public Health 85, no. 8 Pt 1 (Aug. 1995): 1055–58 In some programs, CHWs are employed only for the most complex patients, in partnership with a clinician. In others, community health workers are assigned to less complex patients while referring those with more complex needs to staff with clinical expertise. Some programs use community health workers to provide education and support for chronic health conditions, while others view community health workers as coordinators, without any direct service responsibility.
In most care models, community health workers are assigned to specific populations (children with asthma,(15)J. W. Krieger et al., “The Seattle-King County Healthy Homes Project: A Randomized, Controlled Trial of a Community Health Worker Intervention to Decrease Exposure to Indoor Asthma Triggers,” American Journal of Public Health 95, no. 4 (April 2005): 652–59 women with high-risk pregnancies,(16)S. Redding et al., “Pathways Community Care Coordination in Low Birth Weight Prevention,” Maternal and Child Health Journal 19, no. 3 (March 1, 2015): 643–50. patients with diabetes,(17)M. S. Spencer, K. E. Gunter, and G. Palmisano, “Community Health Workers and Their Value to Social Work.,” Social Work 55, no. 2 (2010): 169–80. etc.) or to specific programmatic aims (e.g., reducing hospital readmissions(18)S. Kangovi, J. A. Long, and E. Emanuel, “Community Health Workers Combat Readmission,” Archives of Internal Medicine 172, no. 22 (Dec. 10, 2012): 1756.). This specificity has emerged as a side-effect of grant-specific aims or, increasingly following the ACA, as a way to reduce high-cost care. Interviewees observed a number of positive outcomes, namely that working with specific populations or toward programmatic goals allows CHWs to have better-defined roles, to receive referrals from other providers, and to be more directed in the services they provide. With clear target populations and tasks, it is easier for community health worker programs to measure success (such as reducing emergency room visits for children with asthma). However, interviewees also expressed concern that the burden on community health workers of intensive documentation of goals can get in the way of their core work.
Community health workers are best integrated into teams when they expand the reach of a practice by working with people that health systems have historically struggled to engage.(19)Payne et al., “Integrating Community Health Workers (CHWs) into Health Care Organizations.” Community health workers often help patients navigate a broad range of health and social needs. This, interviewees noted, is critical for building and maintaining trust with patients.(20)A. Cherrington et al., “Recognizing the Diverse Roles of Community Health Workers in the Elimination of Health Disparities: From Paid Staff to Volunteers,” Ethnicity & Disease 20, no. 2 (2010): 189 When CHWs take on these duties, social workers, nurses, and physicians can operate at the top of their licenses.(21)J. Lloyd and C. Thomas-Henkel, “Integrating Community Health Workers into Complex Teams: Key Considerations,” Center for Health Care Strategies, Inc., May 2017 Directors of successful community health worker programs, as well as the community health workers who participated in our analysis, recommended that health workers spend more time in the community, in line with the origins of the profession, rather than being limited to office work. Interviewees also noted that community health workers (and their supervisors) can be successful in defining roles that complement other team members if the team has good communication protocols and the work is patient-centered. Ultimately, the success of community health workers depends on well-prepared program managers and supervisors who understand and support CHW roles. Many state-based community health worker associations have resource guides for employers seeking to understand how to best utilize CHWs (see Minnesota’s Community Health Worker Toolkit).
Community health workers often address social determinants of health at the local level by acting as community advocates and organizers. As community advocates, CHWs are well positioned to understand and document barriers to healthcare and service gaps. With this documentation, community health workers may be able to elevate concerns to their supervisors, health system leaders, and elected officials. Using their local knowledge and experience, CHWs may also organize their communities to advocate for public policy changes that ultimately improve population health.(22)M. Ingram et al., “A Community Health Worker Intervention to Address the Social Determinants of Health Through Policy Change,” The Journal of Primary Prevention 35, no. 2 (April 1, 2014): 119–23; Pérez and Martinez, “Community Health Workers.” CHW community organizing activities may involve talking with individual patients about barriers to health, soliciting patients’ suggestions for improving their communities, starting community discussions about social factors that affect health, and organizing petitions and meetings to hold elected officials and health systems accountable to their communities.(23)Ingram et al., “A Community Health Worker Intervention to Address the Social Determinants of Health Through Policy Change.” Interviewees noted, however, that advocacy and organizing activities often fall outside of the job description of community health workers in clinical settings, making it hard for CHWs to carry out these activities.
4. Securing sustainable funding for community health workers
Community health workers (CHWs) have historically been funded through time- and resource-limited grants, which interviewees noted can create unsustainable programs that disappear when grants end. However, many healthcare providers and health plans—particularly Medicaid managed care organizations—are becoming interested in CHWs for their potential to improve care quality, increase patient satisfaction, improve patient health, and reduce costs. To demonstrate the financial benefit to Medicaid managed care organizations, many community health worker programs begin by targeting high cost members (e.g. frequent users of the emergency department) or specific populations (e.g., children with asthma(24)Krieger et al., “The Seattle-King County Healthy Homes Project: A Randomized, Controlled Trial of a Community Health Worker Intervention to Decrease Exposure to Indoor Asthma Triggers.” or mothers with high-risk pregnancies(25)Redding et al., “Pathways Community Care Coordination in Low Birth Weight Prevention.”), where reducing costs may be the easiest or have the highest return-on-investment.(26)London et al. describe potential CHW interventions and their financial projections in Connecticut populations where return on investment is likely to be highest. London, Love, and Tikkanen, “Sustainable Financing Models for Community Health Worker Services in Connecticut: Translating Science into Practice.” https://www.cthealth.org/wp-content/uploads/2017/06/CHF-CHW-Report-June-2017.pdf After establishing evidence of cost savings in select populations, however, health plans often lack incentives to extend community health worker services that are simply cost-effective or to work with populations where projected cost-savings extend farther into the future. Below, we describe some of the benefits and drawbacks of different approaches to community health worker funding.
Fee-for-service payments
Interviewees suggested that Medicaid managed care organizations could pay for community health worker services on a fee-for-service basis, like they do for other physician extenders. To use billing codes as a payment system, three notable challenges must be overcome. First, payment rates need to be sufficient to cover costs associated with community-based work, such as travel expenses to visit patients in their homes. Second, community health workers need to be given time to build trust with patients, which often requires that they perform activities that are not amenable to standard codes, such as offering social support during a home visit. Third, codes would direct the work of community health workers toward individual patient activities, while community activities may hold even greater potential for improving overall population health.(27)Wiggins et al., “Preparing Community Health Workers for Their Role as Agents of Social Change.” Nevertheless, some view codes as a necessary bridge to alternative payment models.
Alternative payment models
Those interviewed for the brief described several alternative payment models that may provide incentives for health systems to employ community health workers and may offer sources of sustainable funding in lieu of fee-for-service payments:
- Pay-for-performance models that include bonus payments to providers who meet specified goals and objectives;
- Episode-based payment models that compensate employers that help patients overcome identified risk factors (e.g., inadequate housing);
- Per-member, per-month payments to primary care practices and Medicaid managed care organizations that employ community health workers for care navigation and education support; and
- Tax assessments on health plans or local property taxes, such as in Bernalillo County, New Mexico, that allow regions to employ community health workers.
With State Innovation Model(28)State Innovation Model grant funding was awarded in two rounds, the first in 2013 and the second in 2014. Centers for Medicare and Medicaid Services, “State Innovation Models Initiative: General Information,” https://innovation.cms.gov/initiatives/state-innovations/ resources, a number of states have piloted community health worker programs. Connecticut’s State Innovation Model, for example, uses a shared savings program with “upside-risk” only to encourage employment of community health workers. Vermont’s State Innovation Model funds community health workers by taxing local health providers. A report on Maine’s State Innovation Model described the measurement of social return on investment for CHW models (e.g., reducing missed days of work), which may build an argument for local governments or employers to fund population health-related activities of community health workers in the years ahead.(29)University of Massachusetts Medical School Center for Health Law and Economics, Sustainable Financing Models for Community Health Worker Services in Maine, Nov. 2016: https://commed.umassmed.edu/sites/default/files/publications/Sustainable%20Financing%20ME%20CHWs%20-%20UMass%20Report%20Nov%202016%20Final.pdf
Funding community health workers through alternative payment models may give providers sufficient financial incentives to creatively employ CHWs. However, these arrangements are not without some drawbacks. Healthcare systems, similar to Medicaid managed care organizations, often focus their population health efforts only on their attributed patient population or only on their highest cost patients. This narrow focus creates two challenges. First, health systems might not employ CHWs to do prevention work, such as education for patients who are not high-cost in the short-term. Second, in these settings, CHW roles may be limited to locating patients and making referrals rather than building the trusting, long term relationships that empower patients to better self-manage their health (and that ultimately lower the cost over care over the long term).
Regardless of the payment model, funding community health workers solely through health plans (either by contracting or direct employment) presents several obstacles to CHW sustainability. Perhaps the biggest barrier is that achieving a positive financial return on investments in community health workers may take years and may only be measurable at the population level. By the time an individual health plan achieves cost-savings, the individual patients whose health improved may no longer be covered by the health plan that made the investment.(30)/B. D. Sommers et al., “Insurance Churning Rates For Low-Income Adults Under Health Reform: Lower Than Expected But Still Harmful For Many,” Health Affairs 35, no. 10 (Oct. 1, 2016): 1816–24: https://doi.org/10.1377/hlthaff.2016.0455 In addition, depending on state policy, Medicaid managed care organizations may only be able to pay for community health workers through administrative budgets, which are limited.(31)Health plans must dedicate a specific proportion of their expenditures to services, as opposed to administrative expenses. A ratio of services to administrative expenses for each health plan is calculated, called the medical loss ratio (MLR). Classifying CHWs as an administrative expense disincentivizes plans from investing in CHWs because their MLR will be negatively affected Recent changes to Medicaid managed care rules may make it possible for them to pay community health workers with service budgets, instead of administrative budgets.(32)D. Machledt, Addressing the Social Determinants of Health Through Medicaid Managed Care, The Commonwealth Fund, Nov. 2017 However, many Medicaid managed care organizations work in multiple states, and states often have different regulations regarding community health worker payments.(33)L. M. Gottlieb et al., “Effects of Social Needs Screening and In-Person Service Navigation on Child Health: A Randomized Clinical Trial,” JAMA Pediatrics 170, no. 11 (Nov. 7, 2016): e162521 State policymakers may need to spearhead efforts to solve these and other problems through negotiations with the federal government, state legislatures, and Medicaid managed care organizations.
Due to the variation in CHW care models, the varied interests of healthcare actors, and the dominant fee-for-service payment model, diverse but coordinated funding models may be the best solution. States can issue contracts for community health worker services—both direct services and community-based prevention services. Medicaid waivers could be used to test alternative payment models to sustainably fund community health worker services.(34)For more information on Medicaid waivers, visit: https://www.macpac.gov/subtopic/waivers/ And partnerships between health systems community benefit offices and organizations that offer community health worker services could also be pursued.
Conclusion
Community health workers add value to the healthcare system. More than four decades of research has shown that they play an important role in addressing the social determinants of health and improving health outcomes, particularly among marginalized or other high-risk individuals and communities.(35)Centers for Disease Control and Prevention, Policy Evidence Assessment Report: Community Health Worker Policy Components (Atlanta, GA, 2014): https://www.cdc.gov/dhdsp/pubs/docs/chw_evidence_assessment_report.pdf In recent years, a growing number of health systems have recognized the value of community health workers and have begun to work toward the integration of CHWs into patient care teams. Yet health systems and providers have been slow to fully integrate community health workers into their programs because the strengths and diversity of traditional CHW roles do not easily map to traditional medical care delivery and, most importantly, to existing payment models. Core competency-based training programs, adequate supervision, clear definition of CHW roles, and development and approval of sustainable financing mechanisms are required to tap into the full potential of community health workers.
Acknowledgements: The staff at the Center for Healthcare Research & Transformation would like to thank the Commonwealth Fund for its support of the development of this brief and all the state experts and community health workers interviewed for the brief.
References
| ↑1 | J. Lapedis, E. Kieffer, and M. Udow-Phillips, Revisioning the Care Delivery Team: The Role of CHWs within State Innovation Models (Ann Arbor, MI: Center for Healthcare Research & Transformation, Nov. 2017): Revisioning the Care Delivery Team: The Role of CHWs within State Innovation Models | Center for Health & Research Transformation (chrt.org) |
|---|---|
| ↑2 | L. M. Gottlieb et al., “Effects of Social Needs Screening and In-Person Service Navigation on Child Health: A Randomized Clinical Trial,” JAMA Pediatrics 170, no. 11 (Nov. 7, 2016): e162521, doi:10.1001/jamapediatrics.2016.2521 |
| ↑3 | To date, the most widely used definition is from the American Public Health Association: “A community health worker is a frontline public health worker who is a trusted member of and/or has an unusually close understanding of the community served. This trusting relationship enables the worker to serve as a liaison/link/intermediary between health/social services and the community to facilitate access to services and improve the quality and cultural competence of service delivery.” American Public Health Association, “Community Health Workers,” 2017, https://www.apha.org/apha-communities/member-sections/community-health-workers. |
| ↑4 | E. Rosenthal, C. Rush, and C. Allen, Understanding Scope and Competencies: A Contemporary Look at the United States Community Health Worker Field (University of Texas-Houston School of Public Health, April 2016): http://www.healthreform.ct.gov/ohri/lib/ohri/work_groups/chw/chw_c3_report.pdf |
| ↑5 | A. Olaniran et al., “Who Is a Community Health Worker? A Systematic Review of Definitions,” Global Health Action 10, no. 1 (Jan. 2017): 1272223, https://doi.org/10.1080/16549716.2017.1272223. |
| ↑6 | L. Pérez and J. Martinez, “Community Health Workers: Social Justice and Policy Advocates for Community Health and Well-Being,” American Journal of Public Health 98, no. 1 (Jan. 2008): 11–14: https://doi.org/10.2105/AJPH.2006.100842 |
| ↑7, ↑8, ↑10 | National Academy for State Health Policy, State Community Health Worker Models, National Academy for State Health Policy, Aug. 2017: http://nashp.org/state-community-health-worker-models/ |
| ↑9 | Rosenthal, Rush, and Allen, “Understanding Scope and Competencies: A Contemporary Look at the United States Community Health Worker Field.” |
| ↑11 | N. Wiggins et al., “Preparing Community Health Workers for Their Role as Agents of Social Change: Experience of the Community Capacitation Center,” Journal of Community Practice 21, no. 3 (July 2013): 186–202 |
| ↑12 | For a table outlining the different CHW roles in State Innovation Models across the United States, see our companion brief: J. Lapedis, E. Kieffer, and M. Udow-Phillips, Revisioning the Care Delivery Team: The Role of CHWs within State Innovation Models (Ann Arbor, MI: Center for Healthcare Research & Transformation, Nov. 2017): https://chrt.org/publication/revisioning-care-delivery-team-role-chws-within-state-innovation-models. |
| ↑13 | M. Shah, M. Heisler, and M. Davis, “Community Health Workers and the Patient Protection and Affordable Care Act: An Opportunity for a Research, Advocacy, and Policy Agenda,” Journal of Health Care for the Poor and Underserved 25, no. 1 (2014): 17–24, https://doi.org/10.1353/hpu.2014.0019; J. Payne et al., “Integrating Community Health Workers (CHWs) into Health Care Organizations,” Journal of Community Health, April 8, 2017: https://doi.org/10.1007/s10900-017-0345-4. |
| ↑14 | A. Witmer et al., “Community Health Workers: Integral Members of the Health Care Work Force.,” American Journal of Public Health 85, no. 8 Pt 1 (Aug. 1995): 1055–58 |
| ↑15 | J. W. Krieger et al., “The Seattle-King County Healthy Homes Project: A Randomized, Controlled Trial of a Community Health Worker Intervention to Decrease Exposure to Indoor Asthma Triggers,” American Journal of Public Health 95, no. 4 (April 2005): 652–59 |
| ↑16 | S. Redding et al., “Pathways Community Care Coordination in Low Birth Weight Prevention,” Maternal and Child Health Journal 19, no. 3 (March 1, 2015): 643–50. |
| ↑17 | M. S. Spencer, K. E. Gunter, and G. Palmisano, “Community Health Workers and Their Value to Social Work.,” Social Work 55, no. 2 (2010): 169–80. |
| ↑18 | S. Kangovi, J. A. Long, and E. Emanuel, “Community Health Workers Combat Readmission,” Archives of Internal Medicine 172, no. 22 (Dec. 10, 2012): 1756. |
| ↑19 | Payne et al., “Integrating Community Health Workers (CHWs) into Health Care Organizations.” |
| ↑20 | A. Cherrington et al., “Recognizing the Diverse Roles of Community Health Workers in the Elimination of Health Disparities: From Paid Staff to Volunteers,” Ethnicity & Disease 20, no. 2 (2010): 189 |
| ↑21 | J. Lloyd and C. Thomas-Henkel, “Integrating Community Health Workers into Complex Teams: Key Considerations,” Center for Health Care Strategies, Inc., May 2017 |
| ↑22 | M. Ingram et al., “A Community Health Worker Intervention to Address the Social Determinants of Health Through Policy Change,” The Journal of Primary Prevention 35, no. 2 (April 1, 2014): 119–23; Pérez and Martinez, “Community Health Workers.” |
| ↑23 | Ingram et al., “A Community Health Worker Intervention to Address the Social Determinants of Health Through Policy Change.” |
| ↑24 | Krieger et al., “The Seattle-King County Healthy Homes Project: A Randomized, Controlled Trial of a Community Health Worker Intervention to Decrease Exposure to Indoor Asthma Triggers.” |
| ↑25 | Redding et al., “Pathways Community Care Coordination in Low Birth Weight Prevention.” |
| ↑26 | London et al. describe potential CHW interventions and their financial projections in Connecticut populations where return on investment is likely to be highest. London, Love, and Tikkanen, “Sustainable Financing Models for Community Health Worker Services in Connecticut: Translating Science into Practice.” https://www.cthealth.org/wp-content/uploads/2017/06/CHF-CHW-Report-June-2017.pdf |
| ↑27 | Wiggins et al., “Preparing Community Health Workers for Their Role as Agents of Social Change.” |
| ↑28 | State Innovation Model grant funding was awarded in two rounds, the first in 2013 and the second in 2014. Centers for Medicare and Medicaid Services, “State Innovation Models Initiative: General Information,” https://innovation.cms.gov/initiatives/state-innovations/ |
| ↑29 | University of Massachusetts Medical School Center for Health Law and Economics, Sustainable Financing Models for Community Health Worker Services in Maine, Nov. 2016: https://commed.umassmed.edu/sites/default/files/publications/Sustainable%20Financing%20ME%20CHWs%20-%20UMass%20Report%20Nov%202016%20Final.pdf |
| ↑30 | /B. D. Sommers et al., “Insurance Churning Rates For Low-Income Adults Under Health Reform: Lower Than Expected But Still Harmful For Many,” Health Affairs 35, no. 10 (Oct. 1, 2016): 1816–24: https://doi.org/10.1377/hlthaff.2016.0455 |
| ↑31 | Health plans must dedicate a specific proportion of their expenditures to services, as opposed to administrative expenses. A ratio of services to administrative expenses for each health plan is calculated, called the medical loss ratio (MLR). Classifying CHWs as an administrative expense disincentivizes plans from investing in CHWs because their MLR will be negatively affected |
| ↑32 | D. Machledt, Addressing the Social Determinants of Health Through Medicaid Managed Care, The Commonwealth Fund, Nov. 2017 |
| ↑33 | L. M. Gottlieb et al., “Effects of Social Needs Screening and In-Person Service Navigation on Child Health: A Randomized Clinical Trial,” JAMA Pediatrics 170, no. 11 (Nov. 7, 2016): e162521 |
| ↑34 | For more information on Medicaid waivers, visit: https://www.macpac.gov/subtopic/waivers/ |
| ↑35 | Centers for Disease Control and Prevention, Policy Evidence Assessment Report: Community Health Worker Policy Components (Atlanta, GA, 2014): https://www.cdc.gov/dhdsp/pubs/docs/chw_evidence_assessment_report.pdf |